What Is Lateral Extra-Articular Tenodesis (LET)?
STUDY MATERIAL
PhysioAlchemy
7/24/2025
Here’s the thing: ACL reconstructions aren’t failing because we’re doing them wrong they’re failing because we’re missing something.
That “something” is often rotational stability. And that’s exactly where Lateral Extra-Articular Tenodesis (LET) comes in.
If you’re a physiotherapy student or anyone who plans to treat post-op ACL patients you need to understand LET. Not just the surgical steps, but why it’s done, who benefits most, and what it changes in our rehab approach.
What is LET (Lateral Extra-Articular Tenodesis)?
LET is an additional surgical procedure done alongside an ACL reconstruction to improve rotational control of the knee joint.
Unlike the main ACL graft which is intra-articular (within the joint), LET is extra-articular meaning it works outside the knee joint capsule. It uses a strip of soft tissue (usually the iliotibial band or part of the fascia lata) to reinforce the anterolateral aspect of the knee.
Think of it as a seatbelt. The ACL graft prevents forward translation of the tibia. But the LET acts like a safety harness reducing internal rotation and pivoting movements that stress the graft.
Why is LET Required?
ACL reconstruction alone does a decent job for most athletes. But in high-risk populations like elite footballers, skiers, or younger hypermobile athletes ACL grafts are re-tearing at alarming rates, especially due to uncontrolled rotational forces.
LET is considered when:
There is a high-grade pivot shift on pre-op assessment.
The patient is a high-level pivoting athlete (football, basketball, rugby).
There is generalized ligamentous laxity or genu recurvatum.
It’s a revision ACL reconstruction (previous graft has failed).
There’s damage to anterolateral structures (like the anterolateral ligament, ALL).
Studies show that adding LET to ACL recon significantly reduces the risk of graft re-tear, especially in the first two years post-op.
What Are the Benefits of LET?
Improved Rotational Stability: LET helps control internal tibial rotation and reduces pivot shift. This means less “giving way” and better confidence in cutting, turning, and sudden deceleration.
Lower Re-injury Risk: Athletes with LAET augmentation are less likely to need a revision surgery. Some data shows up to 40–50% reduction in graft failure in high-risk populations.
Better Return-to-Sport Confidence: When you reduce instability, you also reduce fear. LET-supported knees feel more “solid” during play, especially on uneven surfaces or during directional changes.
Protection for the Intra-Articular ACL Graft: By absorbing some of the rotational stress, LET allows the ACL graft to heal in a more stable environment. This may improve the biological incorporation and longevity of the graft.
Surgical Techniques:
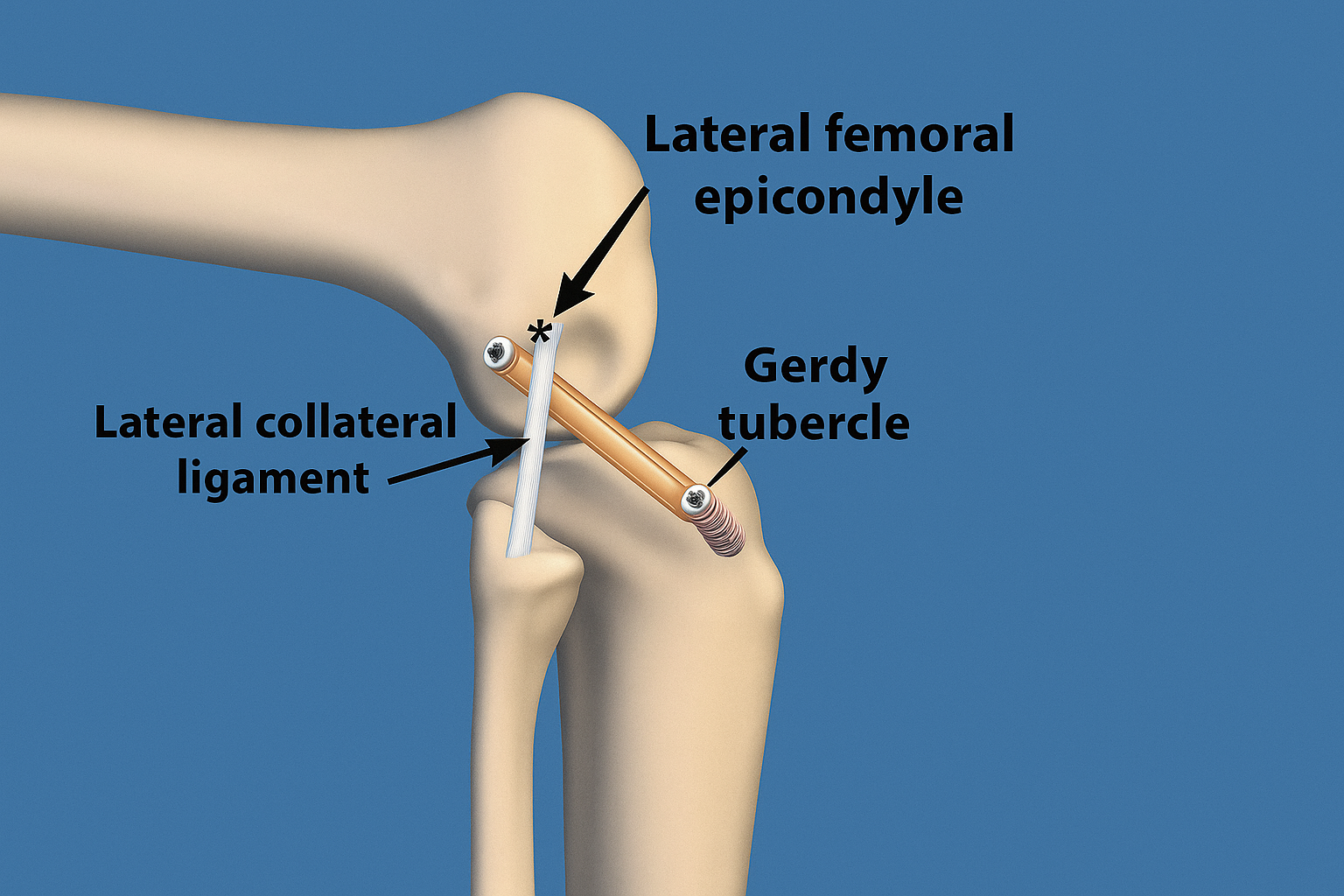
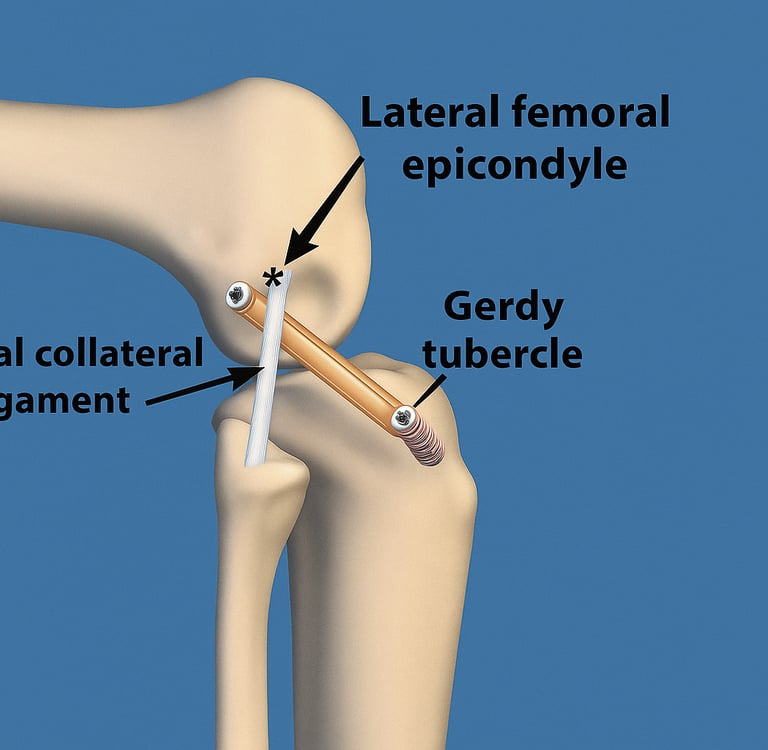
Modified Lemaire Technique is the most common LET method.
A strip of the iliotibial band (ITB) is detached distally, passed deep to the lateral collateral ligament (LCL), and fixed onto the femur.
Some newer techniques use the anterolateral ligament (ALL) concept to target precise rotational control.
Keynotes for Physiotherapy Rehab:
LET changes the biomechanics, healing timeline, and functional progression of post-op rehab. Here’s what you need to keep in mind:
1. Protect Early Healing: Unlike isolated ACL recon, patients with LET might have more lateral discomfort or tightness early on. Avoid aggressive ITB stretching or side-lying leg raises in the first few weeks.
2. Prioritize Gait Training: Watch for subtle compensations. The added lateral tension might slightly affect gait patterns initially. Work on symmetry early and often.
3. Delay Pivoting Drills Slightly: Some protocols suggest delaying cutting and rotational drills by 2–3 weeks compared to standard ACL protocols especially if the patient had significant pre-op instability.
4. Include Proprioception from the Start: Even though you’re avoiding rotation-heavy drills, start with balance and joint position sense training early to retrain neuromuscular control.
5. Communicate With the Surgeon: Always confirm if LET was performed. Rehab can differ significantly depending on whether it's a standard ACLR or an ACL + LET.
Final Thoughts
The future of ACL surgery is not just about fixing the torn ligament but understanding the complex interplay of joint mechanics. LET is a great example of how evolving surgical strategies are making reconstructions stronger and smarter. As a physiotherapy student or professional, being aware of surgical procedures like LET allows you to deliver tailored, intelligent rehabilitation, and bridge the gap between the operating room and return-to-play success.
Your job doesn’t start or end with a protocol. It begins with knowledge and ends with outcomes.