The Shoulder Joint: Anatomy, Biomechanics, and Clinical Relevance
STUDY MATERIAL
PhysioAlchmeny
7/31/2025
Introduction
The human shoulder joint represents one of the most sophisticated designs in the musculoskeletal system. Its hallmark is mobility: it permits a greater range of motion than any other joint in the body. Yet, this mobility comes at the cost of inherent instability, leaving the shoulder vulnerable to both acute injuries and chronic conditions. Clinicians working in physiotherapy, orthopaedics, and sports medicine frequently encounter shoulder dysfunctions that stem from the interplay of anatomy and biomechanics.
Anatomy of the Shoulder Complex
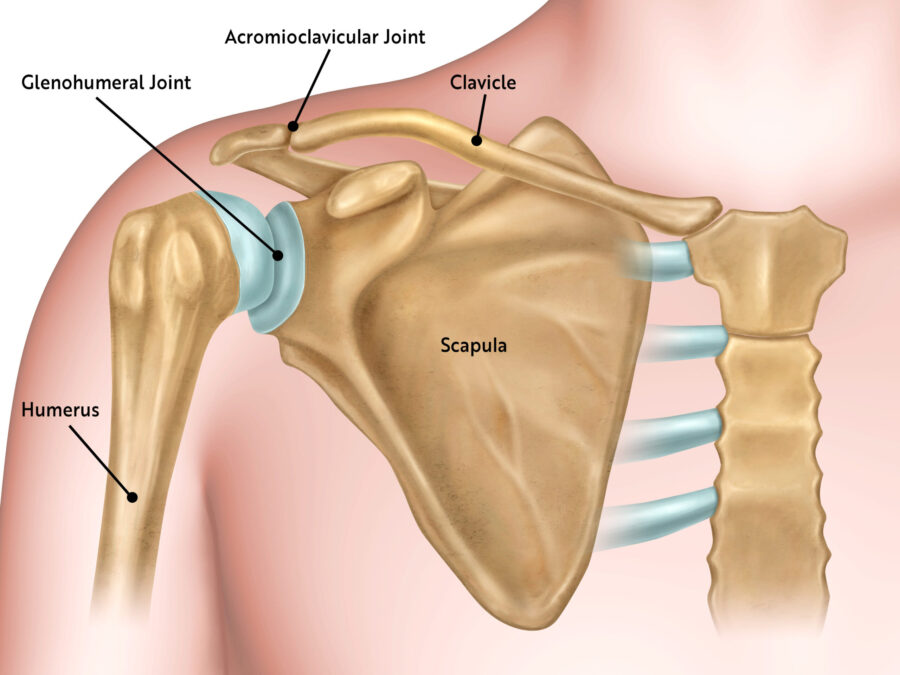
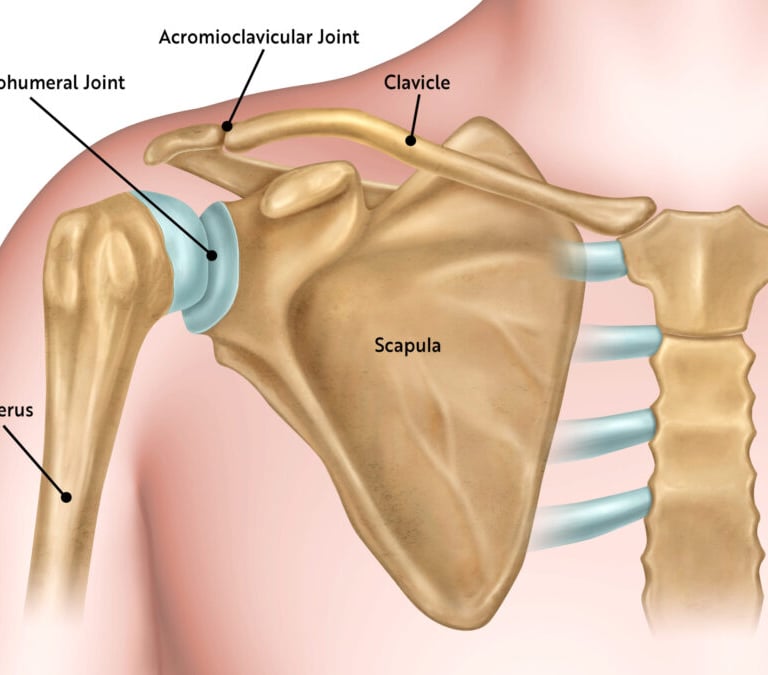
The shoulder is not a single articulation but a complex of four joints working in harmony:
Glenohumeral Joint (GHJ): The ball-and-socket articulation between the humeral head and the glenoid fossa of the scapula.
Acromioclavicular Joint (ACJ): A planar joint connecting the clavicle with the acromion.
Sternoclavicular Joint (SCJ): The only true bony connection between the upper limb and axial skeleton.
Scapulothoracic Articulation (STA): A functional articulation where the scapula glides over the thoracic wall.
Bony Architecture
The humeral head is approximately three times larger than the glenoid cavity, creating a mismatch that favors movement over stability.
The glenoid labrum, a fibrocartilaginous rim, deepens the glenoid socket and improves congruency.
Capsule and Ligaments
The joint capsule is relatively loose, allowing large excursions of the humeral head.
Glenohumeral ligaments (superior, middle, and inferior) provide reinforcement, especially in preventing anterior dislocation.
The coracohumeral ligament supports the superior aspect of the capsule.
Muscular Support
The rotator cuff muscles supraspinatus, infraspinatus, teres minor, and subscapularis play the crucial role of stabilizing the humeral head.
Larger muscles such as the deltoid, pectoralis major, and latissimus dorsi provide power and gross movement.
This intricate network allows the shoulder to combine precision and strength, qualities essential to human dexterity.
Biomechanics of the Shoulder
The biomechanics of the shoulder reflect a delicate balance between mobility and stability.
Range of Motion
The glenohumeral joint permits:
Flexion (0–180°) and extension (0–60°)
Abduction (0–180°) and adduction (0–30°)
Internal (0–70°) and external rotation (0–90°)
Circumduction, a combination of these movements
Scapulohumeral Rhythm
A defining feature of shoulder kinematics is scapulohumeral rhythm. For every 3° of abduction, approximately 2° occurs at the glenohumeral joint and 1° at the scapulothoracic articulation. This coordinated movement prevents impingement of the rotator cuff and maintains optimal muscle length-tension relationships.
Force Couples
Balanced muscle action is essential for stability:
The deltoid elevates the humerus, while the rotator cuff counters superior migration.
The upper and lower trapezius with the serratus anterior create an upward rotation force couple that positions the glenoid optimally during overhead tasks.
Stability Mechanisms
Shoulder stability depends more on dynamic stabilizers (muscles and tendons) than on passive structures (bones and ligaments). Neuromuscular control ensures that the humeral head remains centered in the glenoid during motion.
Clinical Relevance
The unique structure and mechanics of the shoulder predispose it to several pathologies with significant functional consequences.
Impingement Syndrome
Subacromial impingement occurs when the supraspinatus tendon or subacromial bursa becomes compressed beneath the coracoacromial arch. Causes include altered scapular kinematics, weakness of the rotator cuff, or structural variations like acromial spurs. Clinically, patients present with a painful arc between 60° and 120° of abduction.
Rotator Cuff Pathologies
Degenerative changes, overuse, or acute trauma may lead to partial or full-thickness rotator cuff tears. Symptoms include weakness, night pain, and impaired overhead function. Rehabilitation emphasizes strengthening and restoring scapulohumeral rhythm, though surgical repair may be necessary in severe cases.
Shoulder Instability and Dislocation
The shoulder is the most frequently dislocated joint, with anterior dislocation being the most common. Recurrent dislocations can damage the labrum (Bankart lesion) or humeral head (Hill-Sachs lesion). Management may involve rehabilitation focused on proprioception and rotator cuff strengthening, or surgical stabilization.
Adhesive Capsulitis (Frozen Shoulder)
This condition involves progressive capsular thickening and fibrosis, leading to painful restriction of motion in all planes. It is more prevalent in individuals with diabetes mellitus. Physiotherapy focuses on maintaining mobility and minimizing pain, while recovery may take months to years.
Postural and Overuse Syndromes
Modern lifestyles involving prolonged desk work contribute to rounded shoulder posture and altered scapular mechanics. This may lead to muscle imbalances, fatigue, and pain syndromes. Preventive strategies include ergonomic correction, strengthening of scapular stabilizers, and postural training.
Rehabilitation and Clinical Application
Effective rehabilitation of shoulder dysfunction requires integration of anatomical knowledge and biomechanical principles.
Restoration of scapulohumeral rhythm is fundamental in most conditions.
Rotator cuff strengthening ensures dynamic stability of the glenohumeral joint.
Neuromuscular training enhances proprioception and reduces recurrence of instability.
Postural correction and ergonomic adjustments prevent chronic overload.
In surgical cases, physiotherapists play a critical role in graded rehabilitation to restore range of motion, strength, and functional capacity.
Evidence-based protocols now emphasize early controlled mobilization rather than prolonged immobilization to prevent stiffness while still protecting healing tissues.
Conclusion
The shoulder joint exemplifies the intricate balance of mobility and stability in the human musculoskeletal system. Its anatomy provides unmatched versatility, while its biomechanics demand precise coordination of muscles and joints. When this system is disrupted, the clinical consequences can be profound, affecting daily function and quality of life.
For healthcare professionals, particularly physiotherapists, mastery of shoulder anatomy and biomechanics is essential to deliver effective assessment, treatment, and preventive care. As clinical evidence evolves, rehabilitation strategies increasingly highlight the role of dynamic stabilization, neuromuscular training, and patient-specific approaches in optimizing shoulder health.