The Pediatric vs Adult Cardiopulmonary System
STUDY MATERIAL
PhysioAlchemy
8/3/2025
Introduction
The cardiopulmonary system is central to life, delivering oxygen and nutrients while removing carbon dioxide and waste. While adults and children share the same fundamental anatomy, their systems function quite differently. For healthcare professionals, especially those working in rehabilitation or critical care, understanding these differences is key. It shapes how we assess patients, interpret clinical signs, and adapt treatments.
Anatomy and Structural Differences
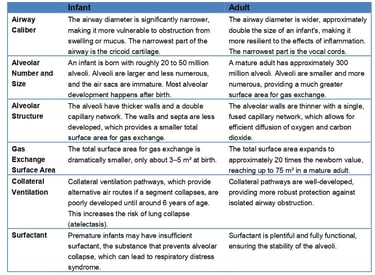
Although the basic structures of the heart and lungs are the same, proportions and mechanics differ significantly between children and adults.
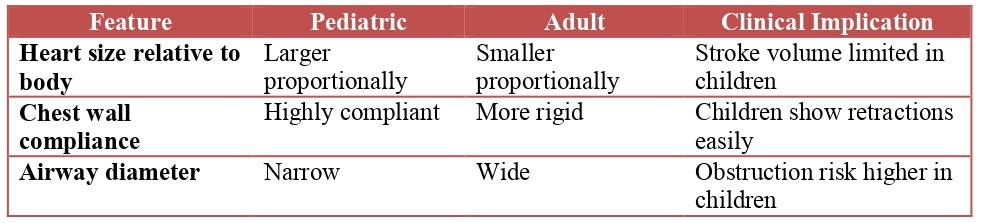
Heart size and position: In infants, the heart occupies a larger proportion of the thoracic cavity. The apex sits more horizontally until the chest elongates with growth.
Chest wall compliance: A child’s rib cage is softer and more flexible, which can exaggerate the appearance of breathing effort during distress.
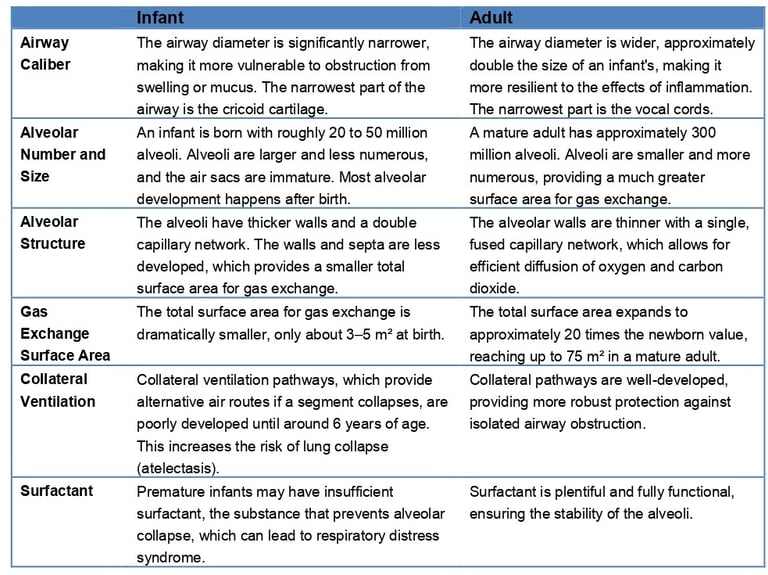
Airway size: Children’s narrower airways mean even small amounts of swelling or mucus can cause significant obstruction.

Physiological Differences
Cardiac physiology
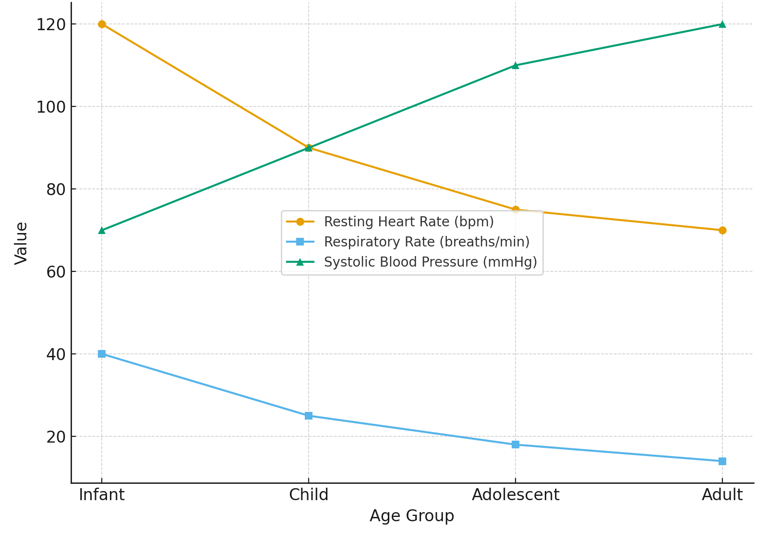
Resting heart rate: Much higher in children to compensate for lower stroke volume.
Stroke volume and cardiac output: Adults can increase stroke volume during exertion. Children rely more on raising heart rate.
Blood pressure: Lower in childhood, increasing gradually into adulthood.
Respiratory physiology
Breathing rate: Faster in children, reflecting higher oxygen demands.
Functional residual capacity (FRC): Lower in children, leaving less oxygen reserve during apnea or distress.
Oxygen consumption: Higher per kilogram of body weight, making children more vulnerable to desaturation.
Developmental Considerations
The cardiopulmonary system does not mature fully at birth. Several developmental features influence how children respond to stress or illness.
Alveolar development: At birth, the lungs have fewer alveoli. These multiply and mature into early childhood, increasing surface area for gas exchange.
Hemoglobin type: Newborns rely on fetal hemoglobin, which binds oxygen more tightly but shifts as adult hemoglobin becomes dominant.
Immune function: Immature defenses leave infants and young children more susceptible to respiratory infections.
Clinical Relevance
Recognizing these differences is essential when providing care.
Exercise tolerance: Children often fatigue faster because of higher metabolic demand and lower oxygen reserve.
Response to illness: Deterioration can be rapid in pediatric patients due to limited compensatory reserves.
Physiotherapy implications:
Breathing exercises should be age-appropriate and often play-based in children.
Positioning can significantly help relieve airway obstruction in children due to their compliant chest walls.
Monitoring must be adjusted to age-specific norms for heart rate, respiratory rate, and blood pressure.
Conclusion
The adult and pediatric cardiopulmonary systems may look alike, but they operate under very different principles. Children’s higher heart rates, faster breathing, and smaller physiological reserves mean they cannot be managed as “small adults.” For clinicians and physiotherapists, keeping these distinctions in mind is crucial for safe and effective practice.