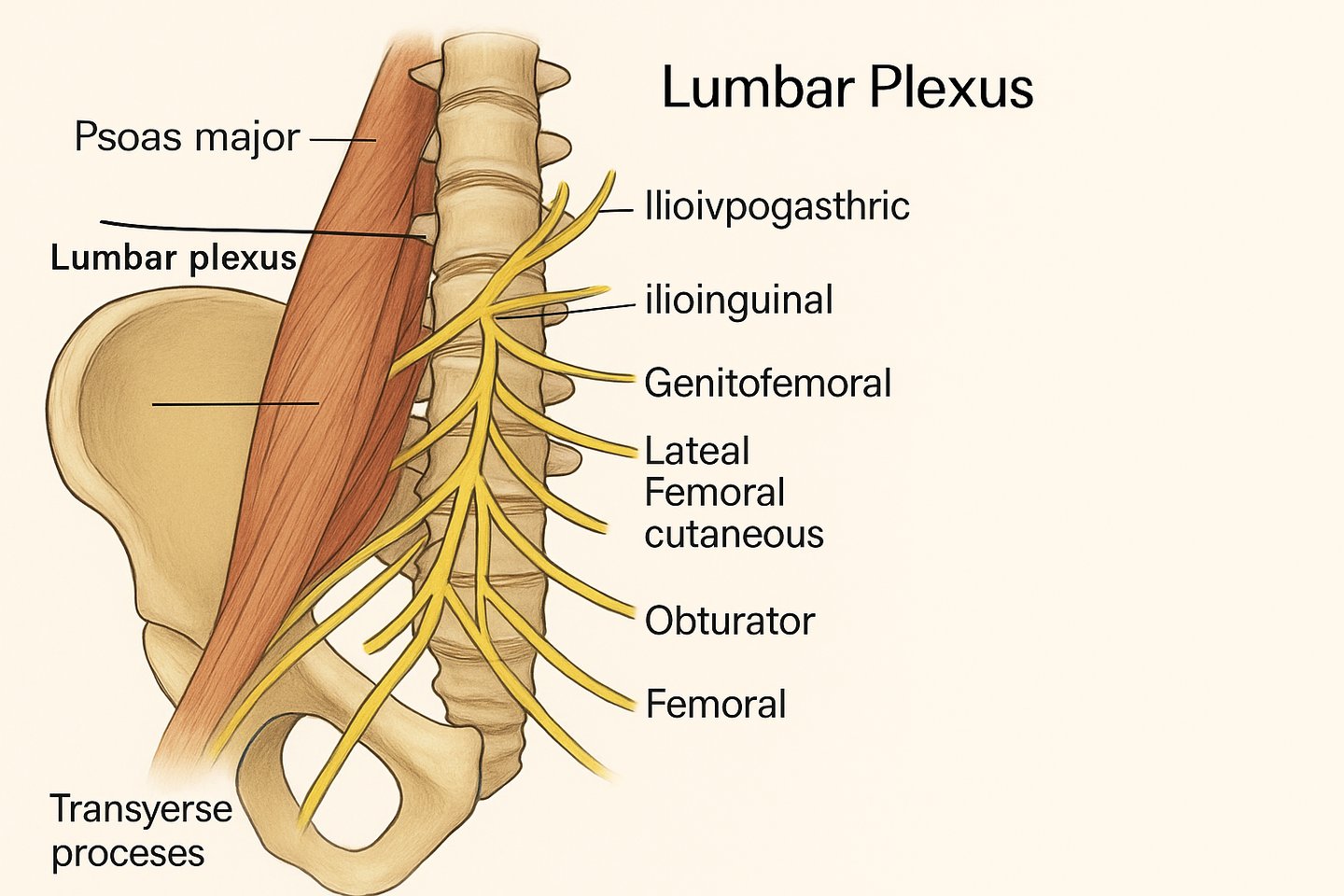
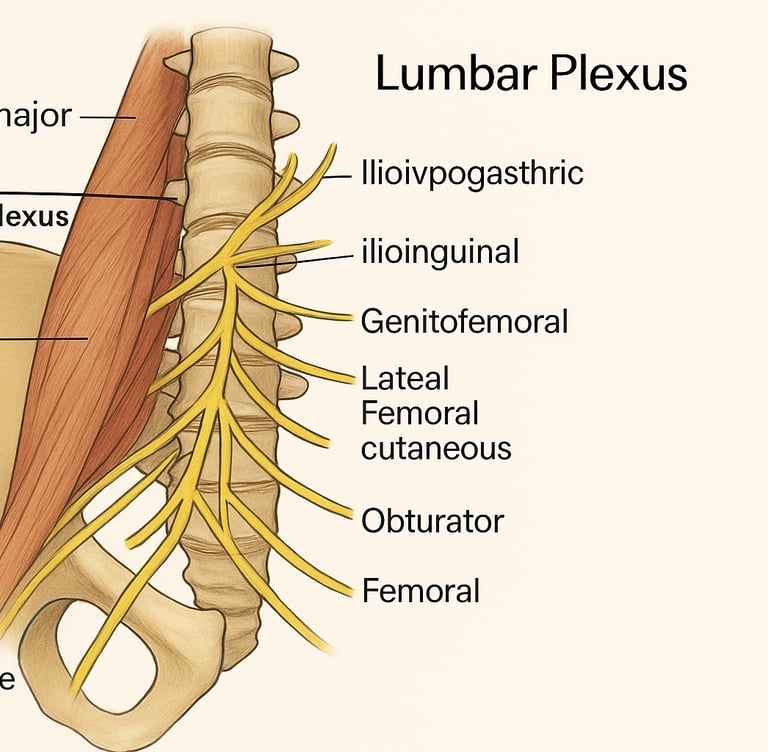
Mnemonic to Remember the Branches (from superior to inferior):
I (Iliohypogastric)
I (Ilioinguinal)
Got (Genitofemoral)
Lazy (Lateral femoral cutaneous)
Over (Obturator)
Flat (Femoral)
Major Branches and Their Functions
1. Iliohypogastric Nerve (L1)
2. Ilioinguinal Nerve (L1)
Motor: Same as iliohypogastric.
Sensory: Skin of the medial thigh, root of penis and scrotum (male), or mons pubis and labia majora (female).
3. Genitofemoral Nerve (L1–L2)
4. Lateral Femoral Cutaneous Nerve (L2–L3)
Passes under inguinal ligament near ASIS.
Sensory: Anterolateral thigh.
Clinical Note: Entrapment = Meralgia paresthetica.
5. Obturator Nerve (L2–L4)
Passes through the obturator foramen.
Motor: Adductor muscles of the thigh.
Sensory: Medial thigh.
Clinical Note: Obturator neuropathy can impair thigh adduction.
6. Femoral Nerve (L2–L4)
Largest branch of the plexus.
Motor: Quadriceps femoris, iliacus, sartorius, and pectineus.
Sensory: Anterior thigh, medial leg (via saphenous nerve).
Clinical Note: Femoral nerve palsy leads to knee extension weakness and loss of patellar reflex.
Relations and Course
The lumbar plexus lies within the psoas major, and its branches emerge either:
Lateral to the psoas: iliohypogastric, ilioinguinal, lateral femoral cutaneous, femoral.
Anterior to the psoas: genitofemoral.
Medial to the psoas: obturator.
Clinical Correlations
1. Nerve Blocks
Lumbar plexus block (psoas compartment block) is used for lower limb surgeries.
Femoral nerve block offers analgesia for anterior thigh and knee.
2. Surgical Risk
Pelvic or retroperitoneal surgeries may damage the plexus (e.g., during lymph node dissection).
3. Psoas Abscess
May compress the lumbar plexus, presenting with pain, weakness, or paresthesia in innervated areas.
4. Diabetic Amyotrophy (Lumbosacral Radiculoplexus Neuropathy)
Presents with asymmetric proximal leg weakness and severe pain.
Involves inflammation of the lumbar plexus in diabetic patients.