Introduction
Cardiac rehabilitation (CR) is more than just recovery it's a structured, science-based journey that helps individuals reclaim their physical, emotional, and social wellbeing after a cardiac event. Whether you've had a heart attack, undergone bypass surgery, or are managing chronic heart failure, CR helps rebuild strength, confidence, and independence under medical supervision.
What this really means is: cardiac rehab is where healing meets movement. It's where you're taught how to live again with awareness, with intention, and with heart.
Who Needs Cardiac Rehabilitation?
CR is prescribed to individuals who have experienced or undergone:
Myocardial infarction (heart attack)
Coronary artery bypass graft surgery (CABG)
Percutaneous coronary intervention (angioplasty with or without stents)
Valve repair or replacement surgery
Heart or heart-lung transplant
Chronic stable angina
Chronic heart failure (especially with reduced ejection fraction)
Even patients with multiple risk factors (diabetes, hypertension, obesity, smoking) benefit from preventive cardiac rehabilitation. The earlier it starts, the better the outcomes.
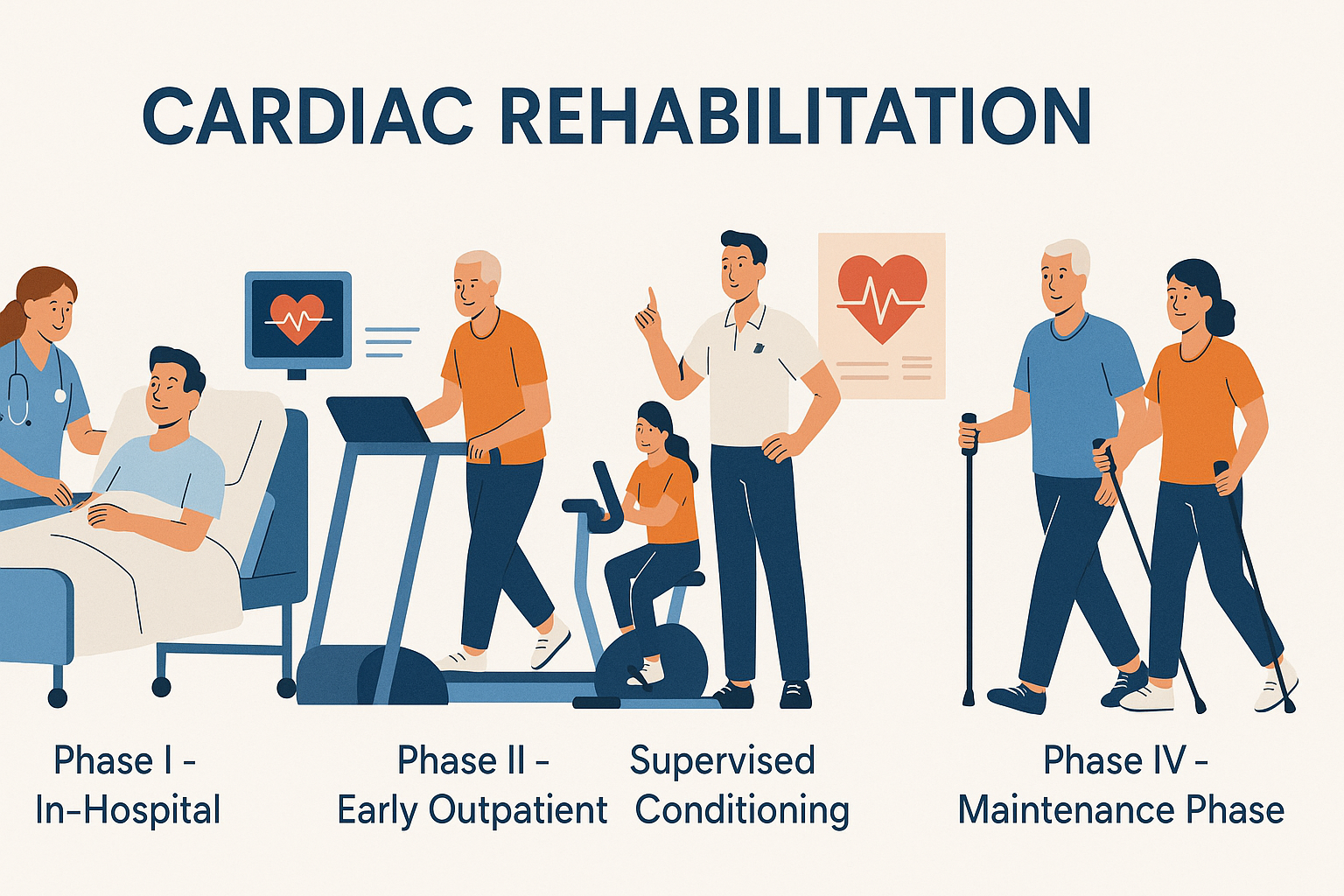
Phases of Cardiac Rehabilitation
CR is classically divided into four progressive phases. Each has a distinct objective, but they all revolve around one principle: safe, progressive return to optimal life function.
Phase I: In-Hospital Phase
Begins during your hospital stay immediately after a cardiac event or surgery.
Goals: Prevent complications, teach energy conservation, introduce mild activity.
Early mobilization: bed mobility, sitting, standing, ambulation within room
Breathing techniques: diaphragmatic breathing, incentive spirometry
Prevent complications: DVT, pulmonary issues, muscle atrophy
Patient & caregiver education: energy conservation, signs of exertion, lifestyle advice
Phase II: Early Outpatient (Supervised)
Usually begins 1-3 weeks post-discharge, in a hospital or clinic setting.
Goals: Improve cardiovascular endurance under supervision, monitor vitals, education on lifestyle.
Continuous ECG monitoring during exercise
Graded aerobic training: treadmill, cycle ergometry, walking
Strength training (light resistance)
Risk factor modification: smoking cessation, medication compliance, dietary education
Psychological support: stress management, relaxation therapy
Phase III: Intermediate Conditioning Phase
Goals: Improve function, restore work capacity, initiate unsupervised training.
More independence with less monitoring
Focused on restoring functional capacity for work or daily life
Group exercise, circuit training, flexibility programs
Integration of psychosocial interventions
Periodic reassessments using 6MWT, METs, RPE scales
Phase IV: Maintenance Phase
Goals: Independent exercise, long-term habit integration, community-based programs.
Community-based or home-based
Emphasizes long-term adherence to healthy habits
Monthly or quarterly follow-ups
Lifestyle coaching, peer support groups
High focus on autonomy, fitness maintenance, and relapse prevention
Benefits of Cardiac Rehabilitation
20–30% reduction in all-cause mortality post-MI or CABG
Decreased hospital readmission
Improved lipid profile, glycemic control, blood pressure
Enhanced peak oxygen uptake (VO2 max)
Reduced depressive symptoms and anxiety
Better adherence to medications and follow-up
Return to work and social engagement
Multidisciplinary Team in Cardiac Rehab
CR is not a one-person show. It requires a coordinated team effort:
Physiotherapist: Leads exercise prescription, functional assessments, vital monitoring
Cardiologist: Medical oversight, medication titration, clearance
Dietitian: Tailors cardiac-friendly diet plans, tracks cholesterol and glucose
Clinical Psychologist: Manages anxiety, depression, stress response
Nurse: Monitors vitals, educates on self-care, ensures medication adherence
Occupational Therapist: Helps in resuming ADLs, work modifications
Role of the Physiotherapist in Cardiac Rehab
As a physiotherapist, you are the bridge between fear and freedom. You help patients trust their body again.
Initial Evaluation: Resting vitals, risk stratification, exercise tolerance tests (6MWT, TMT)
Exercise Prescription:
Intensity: Moderate, based on 40-70% HRR or Borg RPE 11–14
Mode: Aerobic training (walking, cycling, arm ergometer), resistance training
Duration: 20-60 minutes
Frequency: 3–5 sessions/week
Monitoring: BP, HR, SpO2, ECG (when required), subjective symptoms
Education: Energy conservation, body awareness, warning signs
Postural Re-education: Post-surgery (sternotomy precautions), ergonomics
Respiratory Therapy: Incentive spirometry, pursed-lip breathing, thoracic expansion
Functional Goals: Return to work, sexual health, driving, socializing
Red Flags During Cardiac Rehab
Stop exercise immediately if:
Sudden chest pain or tightness
Breathlessness (Borg >5 or SpO2 <90%)
HR increase >20 bpm from baseline without effort
Dizziness or lightheadedness
Excessive fatigue or cold sweats
Systolic BP drop >10 mmHg during activity